Associate Professor College of Medicine, University of Kentucky LExington, United States
Background: This study explores the impact of telehealth on Alzheimer's Disease and Related Dementias (ADRD) patients, focusing on the therapeutic monitoring and medication management of Acetylcholinesterase Inhibitors (AChEIs) such as donepezil, rivastigmine, galantamine, and the NMDA receptor antagonist, memantine.
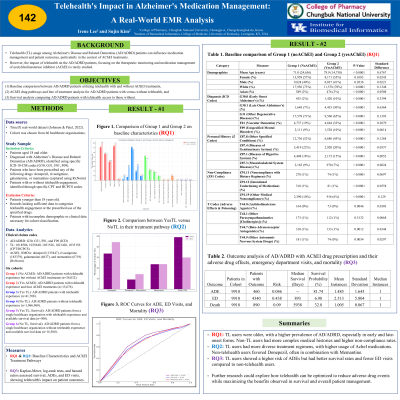
Objectives: The study addressed three research questions: (1) Baseline comparison between ADRD patients utilizing telehealth with and without AChEI treatments, (2) AChEI drug pathways and line of treatment analysis for ADRD patients with versus without telehealth, and (3) Survival analysis comparing ADRD patients with telehealth access to those without.
Methods: Utilizing the TrinetX real-world Electronic Medical Record (EMR) dataset, we conducted a systematic review to explore the impact of telehealth on ADRD patient care. Our analysis involved creating cohorts from four healthcare organizations, encompassing 69,200 ADRD patients selected from a larger dataset of approximately 5.3 million records.
Results: ADRD patients with Telehealth without drug treatments (Group 1=1,400) had a gender distribution of 54% female and 46% male, with an average age of 68.4 years. In contrast, ADRD with Telehealth and drug treatments (Group 2=1,310) showed a slightly different demographic profile with 53% female and 47% male, and a higher average age of 77.6 years. Notably, the prevalence of Alzheimer's disease was 12% in Group 1 and significantly higher at 41% in Group 2. Treatment pathways analysis revealed significant disparities in treatment pathways. For instance, ADRD with Telehealth had a predominant prescription pattern of donepezil (64.32%), followed by memantine (27.67%). ADRD without Telehealth showed a different pattern, with a lower proportion of patients on donepezil (72.04%) and memantine (23.71%). The Kaplan-Meier analysis showed telehealth users in the UK had longer median survival (953 days) and higher survival probability (34.06%) for ED outcomes compared to non-users (886 days, 8.06%), highlighting telehealth's significant survival benefit (p=0.0017).
Conclusions: The data indicate that telehealth usage among ADRD patients can influence medication management and patient outcomes, particularly in the context of AChEI treatments. Telehealth appears to facilitate better management of ADRD, potentially reducing adverse drug events and altering treatment pathways. However, the differential impact on emergency service usage and mortality underscores the complexity of telehealth's role in ADRD care.

.jpg "Irene Lee photo")